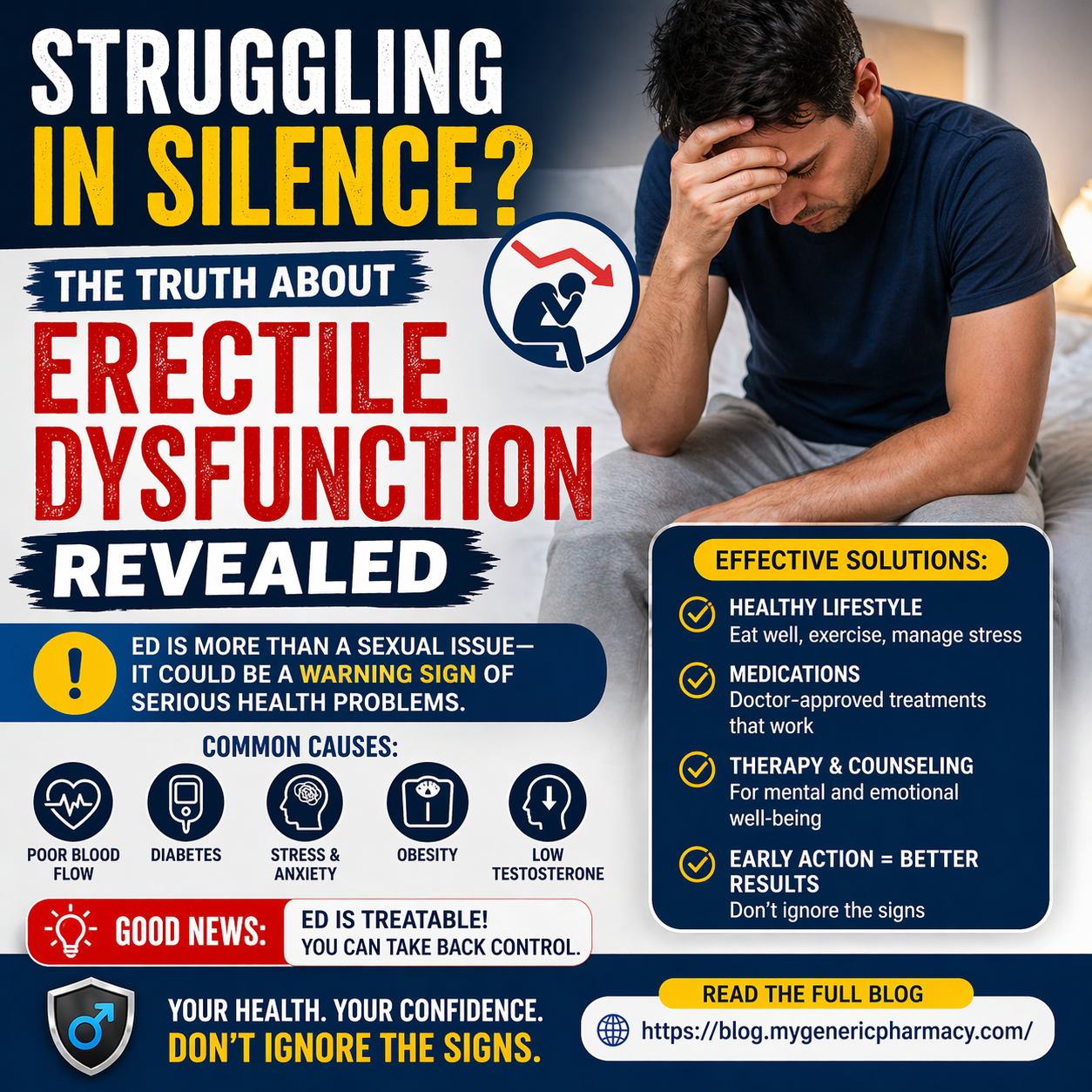
Struggling in Silence? The Truth About Erectile Dysfunction Revealed
Erectile dysfunction is common. However, many people do not talk about it. It affects millions of men around the world. Even so, many men feel shy or embarrassed. As a result, they avoid getting help.
In simple words, Erectile Dysfunction means trouble getting or keeping an erection. At times, this can happen to anyone. However, if it happens often, then it may be a sign of a health problem.
What Is Erectile Dysfunction?
Erectile dysfunction is the inability to get or keep an erection firm enough for sex. In other words, it means the erection is not strong or does not last long enough. At times, men may face occasional difficulty. However, this is normal. But if the problem happens often, then it may be a sign of Erectile Dysfunction.
This condition can affect men of all ages. Even so, it becomes more common with age. However, it is important to note that Erectile Dysfunction is not a natural or unavoidable part of aging. Therefore, men should not ignore it. In fact, many cases can be treated effectively. With the right care and support, improvement is possible.
Common Causes of Erectile Dysfunction
Erectile Dysfunction can have more than one cause. In most cases, it is linked to both body and mind. Therefore, it is important to understand all possible reasons.
Physical Causes
First, physical health plays a big role. Poor blood flow can make erections hard to achieve. For example, these conditions may increase risk:
- High blood pressure
- Diabetes
- Obesity
- Hormone imbalance
In addition, heart problems can reduce blood flow. As a result, erections may become weak or slow.
Psychological Causes
On the other hand, mental health is also important. Stress and anxiety can affect performance. For example:
- Stress
- Depression
- Relationship problems
- Performance fear
Even if the body is healthy, the mind can block arousal. Therefore, mental well-being matters a lot.
Warning Signs You Should Not Ignore
Erectile Dysfunction can start slowly. However, it can also appear suddenly. So, it is important to notice early signs.
Common signs include:
- Trouble getting an erection
- Trouble keeping an erection
- Low sexual desire
- Fear or stress during sex
At first, these signs may seem small. However, they can get worse over time. As a result, they may affect confidence and relationships.
Erectile Dysfunction and Overall Health
Erectile Dysfunction is not just a sexual issue. In fact, it can be a sign of other health problems.
This happens because blood vessels in the penis are small. Therefore, they show damage earlier. As a result, ED may appear before other symptoms.
For example, Erectile Dysfunction may be linked to:
- Heart problems
- High cholesterol
- Diabetes
- Hormone issues
Because of this, early action is very important.
Treatment Options That Work
The good news is that Erectile Dysfunction can be treated. However, treatment depends on the cause.
1. Lifestyle Changes
First, simple habits can help a lot:
- Exercise daily
- Eat healthy food
- Stop smoking
- Limit alcohol
In many cases, these steps improve overall health. As a result, Erectile Dysfunction may also improve.
2. Medicines
Doctors may give medicines to improve blood flow. These can help in many cases. However, always take them with medical advice.
3. Therapy
If the cause is mental, therapy can help. It can reduce stress and improve confidence.
4. Medical Care
In some cases, doctors may suggest other treatments. These include devices or hormone therapy.
Natural Ways to Improve ED
In addition to treatment, natural steps can help.
For example:
- Eat healthy foods
- Keep a healthy weight
- Sleep well
- Reduce stress
Simple habits can make a big difference. However, consistency is key.
Effective Treatment Options for ED
The good news is that erectile dysfunction is treatable in most cases. However, the right treatment depends on the cause. Therefore, it is important to identify the underlying problem first.
1. Lifestyle Changes for ED
To begin with, simple lifestyle changes can make a big difference. For example:
- Regular exercise
- A healthy diet
- Quitting smoking
- Limiting alcohol intake
In many cases, these steps can improve overall health. As a result, they may also improve erectile function.
2. Medications for ED
In addition, medications are commonly used. For instance, Sildenafil (often known as Viagra) helps increase blood flow to the penis. Because of this, it can help achieve and maintain an erection. However, these medicines should only be taken under medical guidance. This ensures safety and proper use.
3. Therapy and Counseling
On the other hand, if the cause is psychological, therapy can be helpful. For example, it can address stress, anxiety, and relationship issues. Moreover, counseling can improve confidence. As a result, it may enhance sexual performance over time.
4. Medical Treatments
In some cases, more advanced treatments may be needed. For instance, doctors may suggest hormone therapy, vacuum devices, or surgery. Therefore, consulting a healthcare professional is essential. They can recommend the best option based on individual needs.
Natural Ways to Improve ED
In addition to treatment, natural steps can help.
For example:
- Eat healthy foods
- Keep a healthy weight
- Sleep well
- Reduce stress
Simple habits can make a big difference. However, consistency is key.
When to See a Doctor
Do not ignore the problem. You should see a doctor if:
- ED lasts for weeks or months
- It affects your confidence
- You have other health issues
Early care can help a lot. In fact, it can prevent serious problems.
Breaking the Stigma
Many men feel shy to talk about ED. However, this should change. ED is a medical condition. It is not a personal failure. Talking to your partner can help. Also, speaking to a doctor can lead to the right treatment. As a result, recovery becomes easier.
Final Thoughts
Erectile dysfunction is common. However, it should not be ignored. In many cases, it is a sign of other health issues. The good news is that help is available. With simple steps, treatment, and support, most men can improve. Start with small changes today. Talk to a doctor if needed. Over time, you can regain confidence and improve your life.
In many cases, early steps can lead to better results. For instance, regular check-ups can help find hidden problems. At the same time, small daily changes can support long-term health. For example, eating fresh foods and staying active can improve blood flow. As a result, the body works better.
References:
- World Health Organization. (2022). Men’s health and noncommunicable diseases.
- Mayo Clinic. Erectile Dysfunction: Symptoms and Causes.
- National Institutes of Health. Erectile Dysfunction Overview.
- American Urological Association. Clinical Guidelines on ED.
- Cleveland Clinic. Erectile Dysfunction: Diagnosis and Treatment.
Medications that have been suggested by doctors worldwide are available on the link below
https://mygenericpharmacy.com/category/mens-health