The Ultimate Seizure Medication Guide: Everything You Need to Know About Anticonvulsants
Seizures can be unpredictable, frightening, and life-disrupting. For millions of people worldwide, anticonvulsants (seizure medications) play a crucial role in managing and preventing these episodes. Whether you’re newly diagnosed or seeking better treatment options, understanding how these medications work can empower you to take control of your health.
In this comprehensive SEO guide, we’ll break down everything you need to know about anticonvulsants—from types and uses to side effects and safety tips.
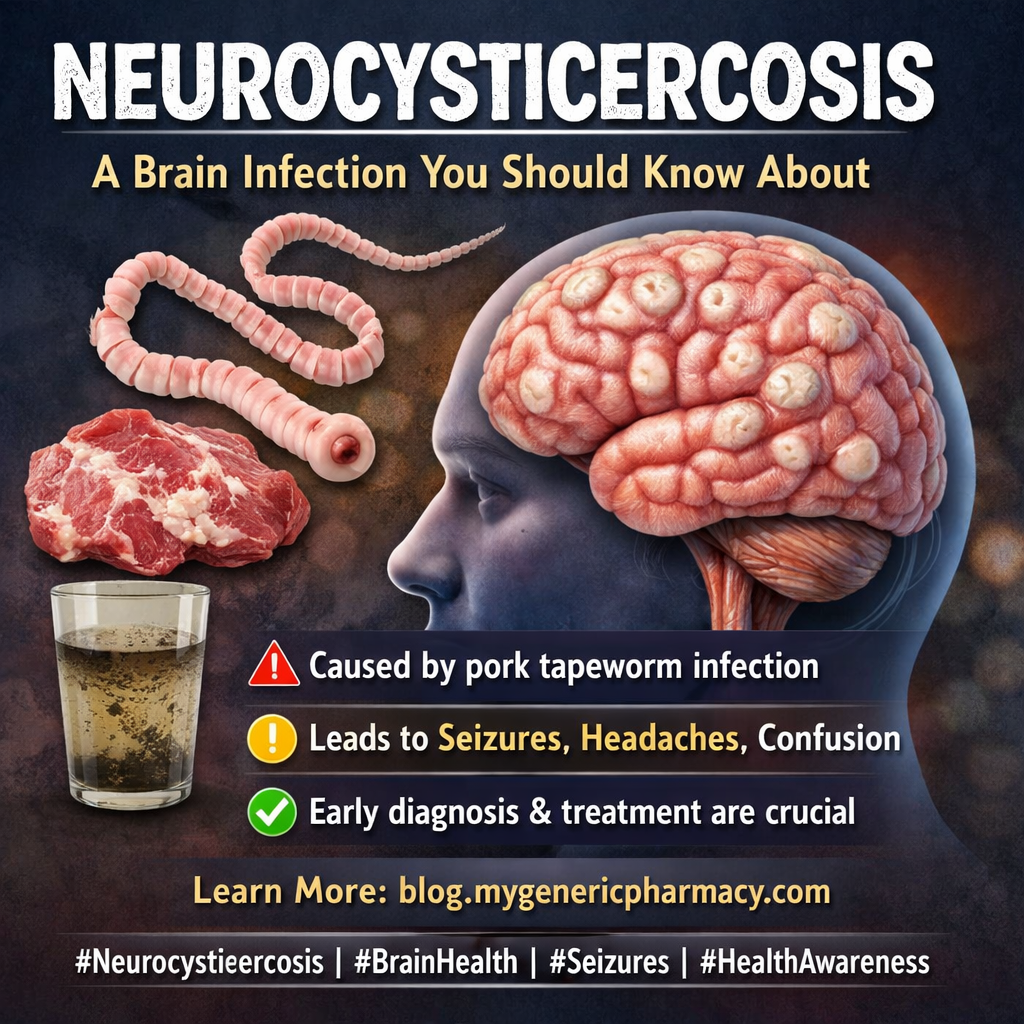
What Are Anticonvulsants?
Anticonvulsants, also known as anti-seizure medications, are drugs designed to prevent or reduce the frequency of seizures. They work by stabilizing electrical activity in the brain, which becomes abnormal during a seizure.
These medications are commonly prescribed for:
- Epilepsy
- Seizure disorders
- Nerve pain (neuropathy)
- Mood disorders (in some cases)
How Do Anticonvulsants Work?
Seizures occur due to abnormal electrical signals in the brain. Anticonvulsants help by:
- Reducing excessive nerve activity
- Enhancing calming neurotransmitters (like GABA)
- Blocking signals that trigger seizures
By restoring balance in brain activity, these medications help prevent sudden and uncontrolled episodes.
Common Types of Anticonvulsants
There are several types of anticonvulsants, and the choice depends on the type of seizure and individual health condition.
1. Broad-Spectrum Anticonvulsants
These treat multiple types of seizures. Examples include:
- Valproate
- Lamotrigine
- Topiramate
2. Narrow-Spectrum Anticonvulsants
These target specific seizure types, such as focal seizures:
- Carbamazepine
- Phenytoin
3. Newer Generation Medications
These often have fewer side effects and improved safety:
Benefits of Anticonvulsant Medications
When used correctly, anticonvulsants offer several important benefits:
- Reduce or completely prevent seizures
- Improve quality of life
- Enable daily activities like work and driving
- Lower risk of seizure-related injuries
Consistency is key—missing doses can increase the risk of seizures.
Possible Side Effects
Like all medications, anticonvulsants may cause side effects. Common ones include:
- Drowsiness or fatigue
- Dizziness
- Nausea
- Weight changes
- Mood swings
In rare cases, serious side effects like allergic reactions or liver issues may occur. Always consult your doctor if you notice unusual symptoms.
Tips for Safe Use
To get the most benefit from your medication, follow these safety tips:
1. Take Medication on Time
Stick to a strict schedule to maintain stable drug levels in your body.
2. Avoid Sudden Stopping
Stopping medication abruptly can trigger severe seizures.
3. Monitor Side Effects
Keep track of how your body responds and report concerns to your doctor.
4. Limit Alcohol
Alcohol can interfere with medication effectiveness and increase seizure risk.
5. Regular Check-Ups
Routine blood tests may be required to monitor drug levels and organ health.
Lifestyle Support for Better Seizure Control
Medication works best when combined with a healthy lifestyle:
- Get enough sleep
- Manage stress effectively
- Eat a balanced diet
- Avoid known seizure triggers
Some individuals may also benefit from specialized diets like the ketogenic diet (under medical supervision).
Seek medical attention if:
- Seizures become more frequent or severe
- You experience serious side effects
- Medication doesn’t seem effective
- You miss multiple doses
Early intervention can prevent complications and improve outcomes.
The Future of Seizure Treatment
Advances in medical research are leading to more targeted and personalized treatments. New therapies aim to reduce side effects while improving seizure control, offering hope for better management in the future.
Final Thoughts
Anticonvulsants are life-changing medications for people living with seizures. Understanding how they work, their benefits, and how to use them safely can make a significant difference in your health journey. With the right treatment plan, lifestyle adjustments, and medical guidance, it is possible to live a full and active life while keeping seizures under control.
References:
https://pmc.ncbi.nlm.nih.gov/articles/PMC11046222/
https://my.clevelandclinic.org/health/treatments/24781-antiseizure-medications-anticonvulsants
https://www.epilepsy.com/tools-resources/seizure-medication-list
https://nurseslabs.com/antiseizure-drugs/
Medications that have been suggested by doctors worldwide are available on the link below
https://mygenericpharmacy.com/category/products/anti-convulsant