Endometriosis: Reason for its prolonged diagnosis.
Endometriosis is a chronic disorder that can produce excruciating pain under various conditions, including menstruation and sexual activity. For some patients, getting an accurate endometriosis diagnosis might be difficult.
According to recent study, a number of factors, including societal and personal barriers, the behaviour and education of healthcare personnel, and other factors, can delay an endometriosis diagnosis by as much as 11 years.

The reasons why getting an accurate endometriosis diagnosis is challenging were recently investigated in a systematic review and qualitative synthesis.
The researchers pinpointed a number of causes, such as the normalisation of menstruation discomfort, the variety of symptoms, and the lack of training and fast referrals among medical personnel.
The analysis highlights opportunities for development in the early diagnosis and subsequent endometriosis treatment.
What is Endometriosis?
According to the Endometriosis Foundation of America, endometriosis is a painful disorder that affects an estimated 200 million people worldwide.
When endometrial-like tissue begins to proliferate outside the uterus, the disorder begins to manifest. Similar tissue normally only develops within the uterus. While it typically affects the rectum and reproductive organs, it can occasionally spread to other sites such as the bowel or pelvic cavity.
Endometrial-like tissue thickens and eventually disintegrates over the course of your menstrual cycle so that it can pass from your body when you menstruate. Similar tissue that develops outside of your uterus and cannot leave your body if you have endometriosis.
It consequently gets caught, irritating the tissues in the area and resulting in scar formation and adhesions. This may lead to chronic pain that gets worse during your period.
Other endometriosis signs and symptoms include:
- uncomfortable urine or bowel movements, especially during your period
- unpleasant interactions
- infertility
- heavy menstrual bleeding
- between periods bleeding
- abdomen and lower back pain right before, during, or right after your period
The following information will help you understand how to diagnose and treat endometriosis.
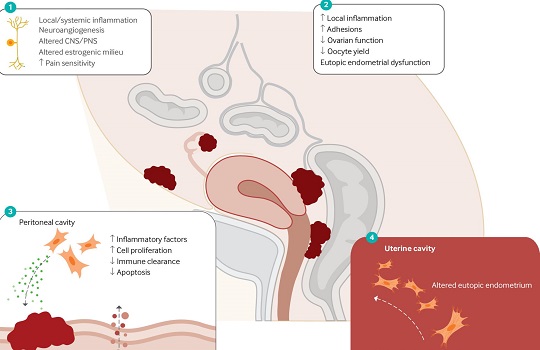
Consequences of endometriosis
In endometriosis, uterine-like tissue develops outside of the uterus. These lesions may be found in the bladder, fallopian tubes, or ovaries, among other places.
Chronic endometriosis is treated mostly by controlling symptoms. Pain, frequently in the pelvic region, is the primary complaint. At some periods, such as during menstruation, the pain could come on. There could be more signs as well, such as exhaustion and trouble getting pregnant. After menopause, endometriosis symptoms may occasionally get better.
Additional information about endometriosis was provided to us by Dr. Ann Peters, an expert in obstetrics and gynaecology at Mercy Medical Centre who was not engaged in the study:
The most common symptom of endometriosis is painful periods, but it can also cause other unpleasant symptoms like heavy bleeding, chest pains, chronic fatigue, diarrhea, and constipation. Other symptoms of endometriosis include pain during sexual activity and during bowel movements.
Endometriosis is thought to affect one in ten women, but there are currently no noninvasive diagnostic methods, such as ultrasound or blood work tests, that would accurately detect endometriosis, according to Dr. Ann Peters.
The authors of the current review observe that a lot of women wait a long time for a proper medical diagnosis. They wished to learn more about the causes of this delay.
Obstacles to diagnosing endometriosis
The 13 articles in this evaluation all complied with the tight eligibility requirements. All of the studies either enrolled endometriosis-affected women or medical professionals with endometriosis diagnosis expertise.
The evaluation concentrated primarily on qualitative research in which individuals talked about their experiences getting an endometriosis diagnosis. The authors’ study of these publications yielded four types of themes that contributed to delayed diagnosis:
- individual elements
- Individual differences
- health system variables
- endometriosis-specific F actors
They discovered that ladies have trouble comprehending the typical menstrual pain on an individual basis. For instance, participants frequently believed that their discomfort was normal and that they should learn to live with it.
The timing of the endometriosis diagnosis was probably impacted by these concepts and the usage of self-care techniques to control symptoms.
Researchers discovered that social stigma against addressing menstrual issues and society’s acceptance of monthly pain as normal may have further delayed diagnosis.
Finally, endometriosis and healthcare circumstances affected when a diagnosis was made. Participants cited instances where general practitioners dismissed concerns or gave the impression that they lacked endometriosis understanding. Similarly, individuals who worked in healthcare said they had received insufficient endometriosis training, and many said they lacked clear clinical guidelines for diagnosis.
There were additional communication issues. Oral contraceptives are occasionally used by medical experts to help diagnose and treat endometriosis. Participants weren’t always given clear explanations of how to rule out other diagnoses or how to utilize oral contraceptives.
Lack of endometriosis testing
Medical specialists also pointed out that endometriosis symptoms often resemble those of other diseases, which can cause delays in diagnosis. Because there are no noninvasive tests that can provide a reliable diagnosis for endometriosis, it might be difficult to make a diagnosis. Referrals were made slowly.
The idea that laparoscopic surgery is the only method of diagnosis was one factor in this. Even medical specialists questioned the value of an endometriosis diagnosis.
Dr. Sophie Davenport, an English physician who wrote the study as part of her Master of Public Health (MPH) dissertation, outlined the multifaceted strategy that will be required to remove these obstacles:
The data’s main takeaways are that there are delays in diagnosis at every stage of the trip. We need to address these on a variety of fronts, from society understanding what “normal” menstruation is and being open to discussing menstrual problems to clinicians being knowledgeable about presentation and diagnosis and paying attention to patients who claim their periods aren’t normal, according to study author Dr. Sophie Davenport.
Diagnosed with endometriosis in the past
There were some issues with this study that point to the need for more investigation.
All of the research in the study were carried out in high-income nations, the majority of which provided universal healthcare. As a result, it might not be able to generalize the findings, and this research doesn’t address any potential financial obstacles to diagnosis.
The majority of participants in studies that provided demographic data were white women, highlighting the need for increased diversity in future research.
The samples among participants with endometriosis may be biassed towards those with more severe cases.
Participants in the research that examined the opinions of healthcare professionals were mostly general practitioners and doctors. Other service providers and experts in the field could be studied in future studies. The review was undertaken by just one reviewer, which increased the chance of bias or methodological flaws.
Dr. Davenport identified the following areas of future study:
Investigating how a patient’s perceptions of receiving an endometriosis diagnosis vary now that the clinical guidelines advise treating empirically based on signs and symptoms rather than doing a laparoscopic surgery first will be an important topic of research. According to the papers, this discouraged physicians from sending women to specialty services and caused a delay in the diagnosis and subsequent treatment of those women, according to Dr Sophie Davenport.
Can I speed up the diagnosing process?
It is becoming simpler to receive a correct diagnosis as more individuals become aware of endometriosis and its symptoms. However, there are a few things you can do ahead of time to make sure you receive a prompt, correct diagnosis:
Try a self-test for endometriosis. Here is a quiz you can give yourself. on show your doctor during your appointment, print out your results, or save them on your phone.
Maintain a symptom log. Keeping thorough records of your symptoms may seem boring, but they will help your doctor make a proper diagnosis. Record your symptoms’ severity on a scale of 1 to 10, as well as any details about when in your cycle they often appear.
Use a period-tracking app or a notebook to record this information.
Find a specialist in endometriosis. Request a recommendation from your doctor for a gynecologist who specializes in endometriosis. For doctor recommendations and other advice, you can also look through internet support communities.
REFERENCES:
- https://www.healthline.com/health/endometriosis-diagnosis
- https://www.medicalnewstoday.com/articles/why-does-receiving-diagnosis-endometriosis-take-so-long
- https://www.forbes.com/sites/alicebroster/2020/08/27/why-it-takes-so-long-to-be-diagnosed-with-endometriosis-according-to-a-expert/
- https://www.everydayhealth.com/hs/womens-health/endometriosis-diagnosis/
For Sexual disease medications that have been suggested by doctors worldwide are available here https://mygenericpharmacy.com/index.php?therapy=24